
Cyclicity and energy
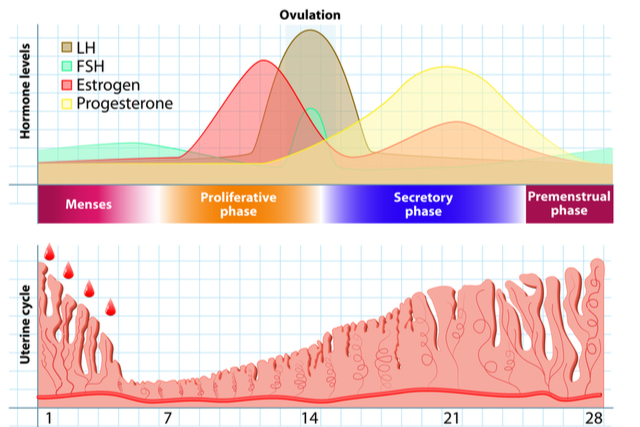
The menstrual cycle is made up of four phases: menstruation, the follicular phase, ovulation and the luteal phase. This continuous cyclical regression and renewal is energetically costly and maintains the endometrium in a metabolically active state to synchronize with implantation. The menstrual cycle changes pace to maintain women’s fitness and control fecundity.
What is the Luteal Phase?
The luteal phase begins during the second half of a cycle as the mature egg which has ovulated starts travelling down the fallopian tube. This phase normally (not always) lasts around 12-14 days after ovulation and ends when the period begins.
When the ovarian follicle has released its egg, the follicle itself changes, the empty sac closes off, turns yellow, and transforms into a new gland called the corpus luteum. The corpus luteum, from which the phrase “luteal phase” originates, is responsible for producing progesterone and some oestrogen. During the luteal phase, progesterone thickens the lining of the uterus so that a fertilized egg can implant. Blood vessels grow inside the lining and supply oxygen and nutrients to the developing embryo.
Progesterone levels rise throughout pregnancy. A general guide is shown below.
| first trimester | 10 to 44 ng/mL of progesterone |
| second trimester | 19 to 82 ng/mL |
| third trimester | 65 to 290 ng/mL |
If a fertilized egg is not present or the levels of the hormones are not optimal, the corpus luteum will shrink and die, forming a tiny piece of scar tissue and progesterone levels will drop. The uterine lining will shed during menstruation. The entire cycle is then repeated.
Length of the luteal phase
In most women, the luteal phase lasts 12 to 14 days. It is considered to be short if it lasts less than 10 days. This short luteal phase prevents the uterine lining having the opportunity to grow and develop enough to support a growing baby. As a result, it can be harder to get pregnant or it might take longer to conceive. A short luteal phase can be a sign of a condition called luteal phase defect (LPD).
Luteal Phase Defect
Luteal Phase Defect or LPD is where there is an abnormality in the endometrial development. When suspected luteal phase defect occurs, the secretion of progesterone by the ovary is below normal or the endometrium does not respond to the normal stimulation of progesterone. This luteal phase defect is associated with both infertility and early miscarriage.
Do I have Luteal Phase Defect?
- Is your luteal phase less than 12 days long?
- Do you have vaginal spotting before you get your menstrual bleed? It is often a symptom of a low level of progesterone.
- Have you noticed a slow or low rise on your basal body temperature (BBT) chart following ovulation? Woman’s BBT averages between 36.1°C and 36.4°C. After ovulation, it rises to 36.4°C to 37°C. Look for this temperature bump to inform you that you’ve ovulated and entered the luteal phase.
- Do you have an adequately thick endometrial development? Once the proliferative phase of the menstrual cycle (days 6–14) begins, the endometrium becomes thicker (5–7 mm) reflecting the development of glands, blood vessels, and stroma. Around ovulation, the endometrium develops a multilayered appearance which can measure up to 11 mm in thickness. The layered appearance usually disappears 48 hours after ovulation. During the secretory phase, the endometrium becomes even thicker (7–16 mm) reaching a maximum thickness during the mid-secretory phase.
- Did you have a day 21 blood test to check progesterone level? A level of less than 10 nanograms may indicate a problem.
In western medicine, LPD is often treated using clomiphene citrate to stimulate follicular growth, but due to its anti-oestrogen effect, the endometrial lining becomes thin. My article on Clomiphene citrate is here. Use of supplemental hCG or additional progesterone has limited success. Hormones never act in isolation as they continuously and sensitively interact with the totality of one’s internal chemistry and energy availability.
Eastern Medicine perspective on Luteal Phase Defect
Luteal phase defect has been a historically well-documented entity in fertility care in Eastern Medicine. Often called as ‘Kidney deficiency’, LPD has been classified according to symptoms and signs and individual constitutions. Categories of composite medicine have been established to improve ovarian function, fertility and prevent miscarriage. Specific herbal medicine that tonifies (energizes) the kidney/reproductive system and regulates the menstrual cycle has shown such properties.
Studies have demonstrated that the herbal medicine treatment traditionally utilized to treat LPD and regulate the menstrual cycle has resulted in improved biomarkers such as increased BBT and hyperthermal phase after ovulation or a remarkably shortened transitional period of BBT. Pregnancy was achieved in 56% of the LPD cases.
At Pathways, we support those with LPD with personalized medicine. Where conception is delayed and miscarriage has occurred, we promote ovarian function and angiogenesis to improve endometrial receptivity.
Dr Ryu’s articles
Improving Endometrial Receptivity for IVF success
Endometrial Receptivity and Implantation
Angiogenesis: Can you make new blood vessels?
The role of Angiogenesis in Reproduction



